In May 2025, the Centers for Medicare & Medicaid Services (CMS) announced a radical overhaul to the way the agency oversees Medicare Advantage (MA) plans.
Among other changes, CMS stated it would expand risk adjustment data validation (RADV) audits to all Medicare Advantage contracts and compress review of Payment Years 2020 through 2025 into approximately 18 months.
Background of RADV audit changes
The announcement was the result of converging factors:
1. First, CMS periodically revises its risk adjustment strategy to contend with economic developments in Medicare Advantage, as well as to respond to previous audit findings by CMS and by the Office of the Inspector General in the Department of Health and Human Services (HHS-OIG).
2. Second, the increasing costs of healthcare have put increasing political pressure on subsequent administrations to curb costs for both consumers and the government.
>>Learn more about the changes to CMS RADV audits.
CMS RADV schedule: The accelerated “catch-up” period
At the time of the 2025 announcement, CMS was still facing a backlog of payment year audits: RADV audits for Payment Year 2019 through PY 2024 had not yet been audited. As part of its overhaul, CMS vastly expanded its auditor workforce and initiated an accelerated series of non-sequential Payment Year audits to clear the backlog.
The announced schedule is structured as follows:
According to this schedule, a new payment year audit begins approximately every three months. The submission window for plans to respond with validation evidence, however, is five months—which means payment year audits overlap, as depicted in the chart below.
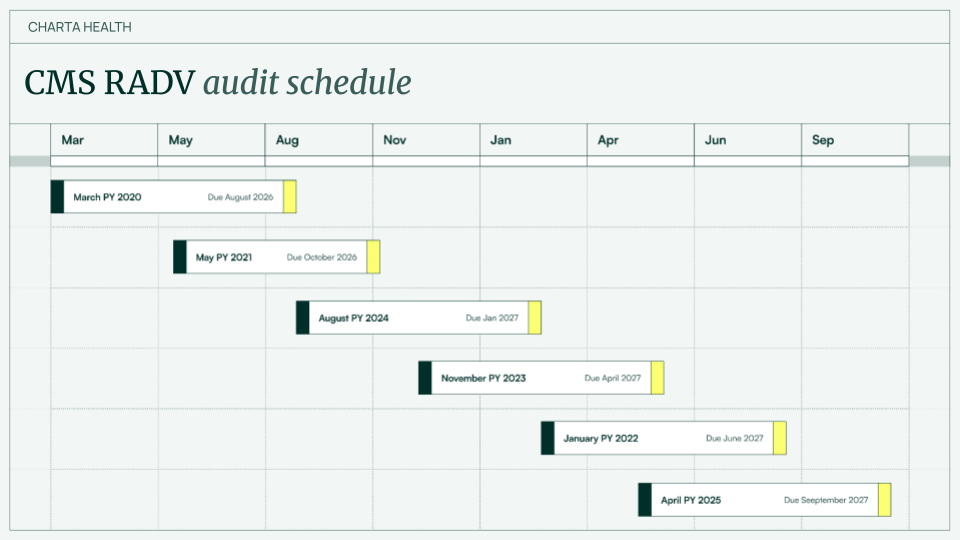
For plans with multiple contracts extending across multiple payment years, the operational resources required for audit response are now multiplied by a significant factor—making modern technology for HCC validation exercises a priority across plans.
CMS RADV audits: Looking ahead
By the time CMS initiates PY 2025 audits in April 2027, the agency will have normalized a more timely lookback on risk adjustment data.
For MAOs, surviving the compressed, high-velocity enforcement environment will require shifting from a reactive "audit response" posture to a proactive, continuous compliance model.
Ensuring that robust, defensible clinical evidence backs every HCC is no longer a best practice for avoiding potential recoupments deriving from periodic inspection: It’s necessary for a plan to avoid punitive actions resulting from guaranteed scrutiny.
.png)